
Translate this page into:
Diphtheritic tonsillitis in an immunized adult: A case report

*Corresponding author: Tessa Antony, Department of Microbiology, Sri Ramachandra Medical College and Research Institute, Chennai, Tamil Nadu, India. drtessa@sriramachandra.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Avinash S, Antony T, Somu L, Selvin Gnanadas SQ. Diphtheritic tonsillitis in an immunized adult: A case report. Sri Ramachandra J Health Sci 2023;3:25-7.
Abstract
Corynebacterium diphtheriae is a Gram-positive bacillus which can be either toxigenic or non-toxigenic depending on the production of the diphtheria exotoxin. Diphtheria is a potentially fatal infectious disease caused by toxigenic strains of C. diphtheriae. Despite the national immunization program, India accounts for approximately 20% of the total cases according to the recent World Health Organization reports. Even though it is a vaccine preventable disease, cases are being reported, which may be due to lack of booster doses or waning of immunity with increasing age. Here, we report a case of diphtheritic tonsillitis in a 30-year-old immunized adult who came to the otorhinolaryngology outpatient department with acute onset of throat pain and difficulty in swallowing. C. diphtheriae was isolated from bacteriological culture of throat swab. The patient was symptomatically better with 2 weeks of treatment with oral erythromycin 500 mg twice a day.
Keywords
Corynebacterium diphtheriae
Diphtheria
Immunization

INTRODUCTION
Diphtheria is an acute infectious disease of childhood caused by Corynebacterium diphtheriae. C. diphtheriae causes noninvasive localized infection of primarily respiratory tract and skin. Symptoms of infection at distant sites can occur due to absorption and dissemination of diphtheria exotoxin through the bloodstream that can lead to complications such as myocarditis and polyneuritis.[1] The mode of transmission is by direct contact or by inhalation of aerosolized secretion from the infected individual. Respiratory diphtheria is one of the most common presentations of this infection, which is characterized by the presence of a pseudomembrane over the tonsil. The incidence of respiratory diphtheria has come down due to effective vaccination while the incidence of cutaneous diphtheria is more due to the emergence of non-toxigenic strains.[2] The sites involved in respiratory tract infection include anterior nasal, faucial, laryngeal, and tracheobronchial region. The most common site is faucial which is characterized by sore throat, low-grade fever, and pseudomembrane over the tonsils and pharynx. Here, we report a case of diphtheritic tonsillitis in an immunized adult.
CASE REPORT
A 30-year-old female presented to the otorhinolaryngology outpatient department with complaints of throat pain for 10 days which was sudden in onset and progressive in nature. She also complained of difficulty in swallowing for 10 days for both solids and liquids. She had no complaints of fever, breathing difficulty, or neck swelling. She was fully vaccinated in childhood according to the universal immunization schedule, as confirmed by her mother. On general examination, the patient was oriented to time, place, and person. On physical examination, there was left jugulodigastric node enlargement and there was no pallor, icterus, clubbing, cyanosis, lymphadenopathy, or pedal edema. Her pulse rate was 84 beats/min, and her blood pressure was 110/70 mmHg. Throat examination revealed bilateral Grade I tonsillar enlargement with a membrane over it and a clear posterior pharyngeal wall, no diffuse swelling of the neck. The condition was provisionally diagnosed as tonsillitis and throat swab from the patient was sent to the microbiology laboratory. Gram staining was performed which revealed epithelial cells and Gram-positive bacilli with no inflammatory cells [Figure 1]. Bacteriological culture was made on 5% sheep blood agar, chocolate agar, and potassium tellurite agar and incubated aerobically at 37ºC. Black colonies grew on potassium tellurite agar on the 3rd day of incubation [Figure 2]. Gram stain from the colonies grown showed Gram-positive bacilli in cuneiform arrangement [Figure 3]. Albert stain from the colonies showed green-colored bacilli with bluish-purple metachromatic granules [Figure 4]. The isolated colony was identified further using matrix-assisted laser desorption ionization-time of flight mass spectrometry (VITEK®MS, bioMeriuex, Sweden), and the organism was identified as C. diphtheriae. The isolate was further sent to Christian Medical College, Vellore for toxin detection. It was found to produce toxin by Elek’s gel precipitation test. The isolate was found to harbor tox a gene by polymerase chain reaction. Before the laboratory confirmation of C. diphtheriae, the patient was started on oral amoxycillin clavulanic acid 625 mg twice a day (Tab Augmentin 625 mg). After the diagnosis of diphtheritic tonsillitis, the patient was admitted to an isolation room and droplet precautions were followed. According to clinical laboratory standard institute M45 guidelines, broth microdilution is the recommended antimicrobial susceptibility testing method, which could not be performed for this isolate. The patient was further treated with oral erythromycin 500 mg twice a day for 14 days as per recommended guidelines. The patient improved symptomatically and was discharged. On further follow-up after 2 weeks, the patient was found to be asymptomatic and repeat throat swab culture was negative for C. diphtheriae.
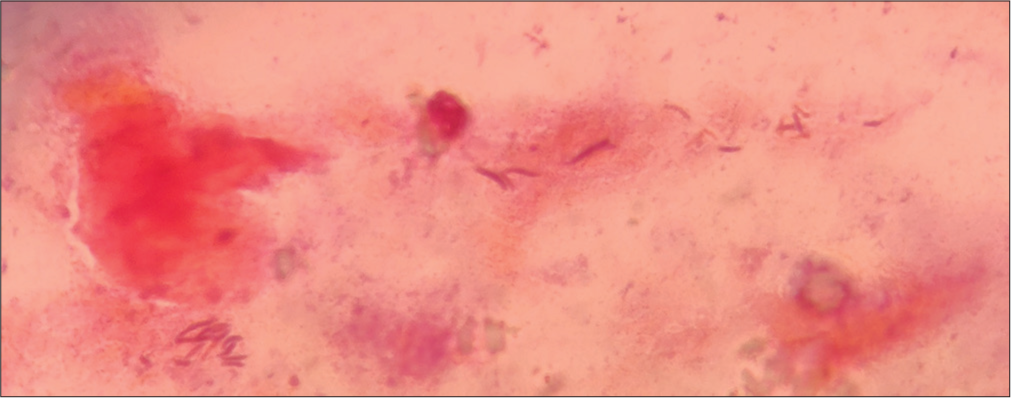
- Gram stain of throat swab showing Gram-positive bacilli.
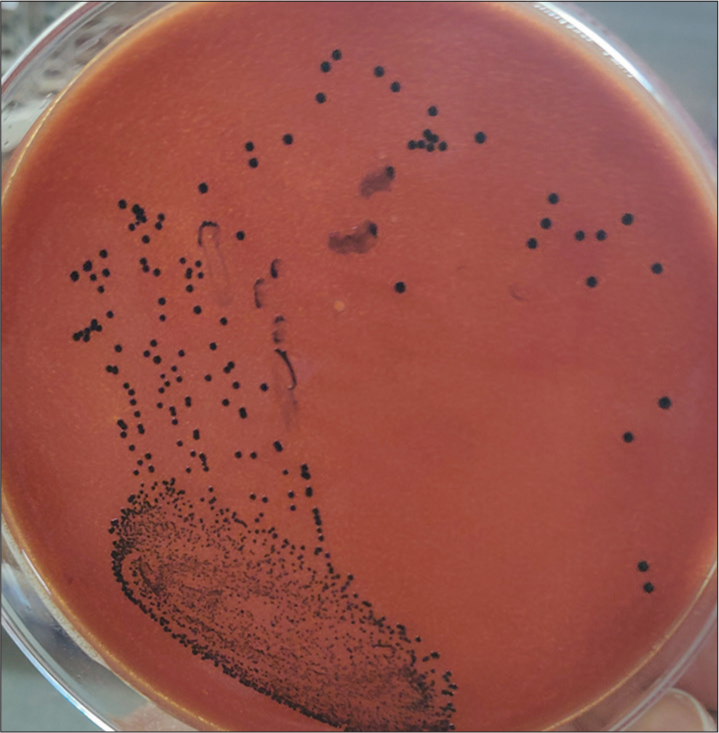
- Black colonies of Corynebacterium diphtheriae on potassium tellurite agar.
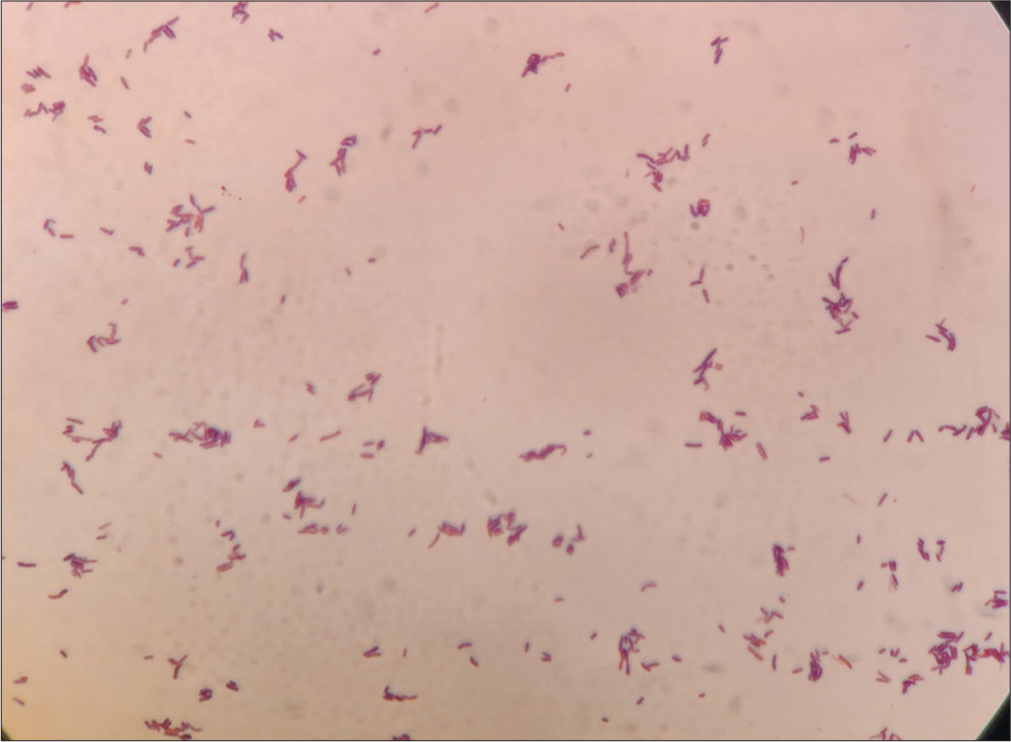
- Gram stain from the colonies showed Gram-positive bacilli in cuneiform arrangement.
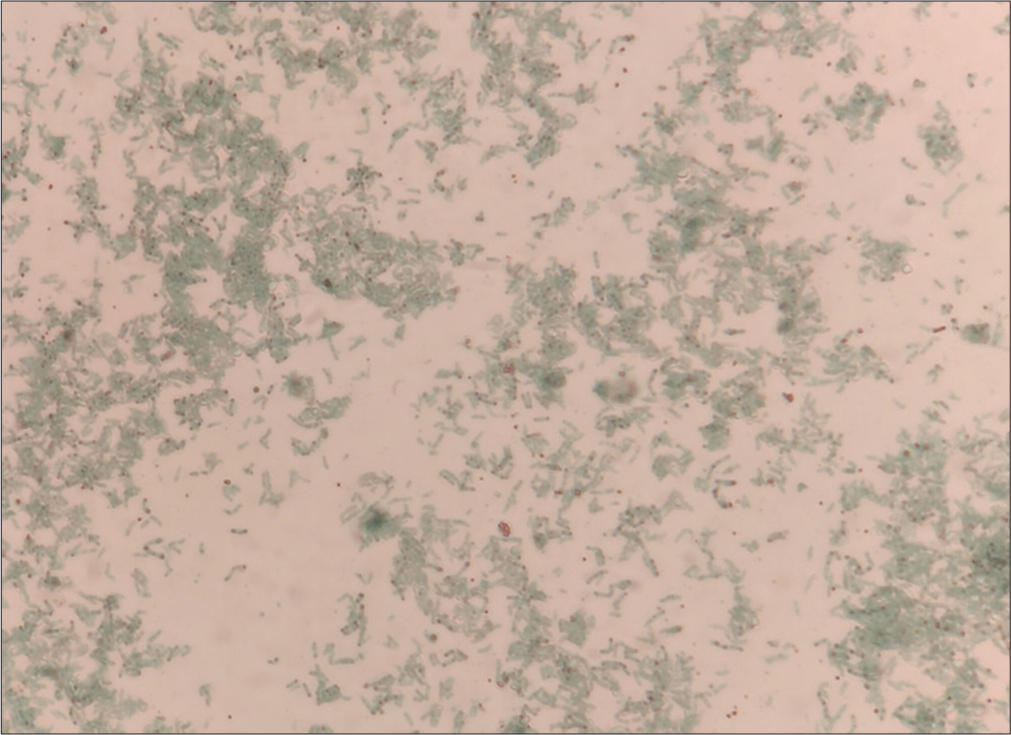
- Albert stain from the colonies showed green-colored bacilli with bluish-purple metachromatic granules.
DISCUSSION
Despite diphtheria being a vaccine-preventable disease, there is a re-emergence of this infection. Globally, according to the World Health Organization 8638 people are infected with diphtheria in 2021 and India has reported 1768 cases which account for approximately 20% of the total cases.[3] The case fatality rate is 5–10% and higher rates are reported in children.[4] The case fatality ratio was low due to active surveillance during the outbreak along with prompt diagnosis, isolation, and treatment of cases and as well as contacts.[5] Although the diagnosis of diphtheritic tonsillitis can be made clinically, the microbiological diagnosis should also be done to differentiate it from severe streptococcal throat infection. To prevent toxin-mediated complications and also further transmission, anti-diphtheritic serum and antibiotic therapy are usually administered to the patient. Effective antibiotics for treatment of diphtheria include penicillin, erythromycin, clindamycin, and tetracycline. However, the recommended drug of choice is erythromycin 500 mg twice a day for a duration of 14 days.[6]
In the present case, the patient was a 30-year-old female and the age shift from children to adolescents and adults has been reported from several states in India.[7] The main source of infection in the community is unimmunized children.[8] In the national immunization schedule, three doses of diphtheria vaccine are administered at 6, 10, and 14 weeks of age followed by two booster doses at 2 years and 5 years of age. Despite effective vaccination, the patient acquired diphtheria, probably due to waning immunity. Increased susceptibility risk in adults occurs due to the infecting dose, virulence of the diphtheria bacilli, and overcrowding.[9] Disease in previously immunized individuals is mild and less likely to be fatal. This could have been the reason why the patient did not suffer any symptoms related to the toxin, even though she had infection with a toxigenic strain. The re-emergence of diphtheria in adults can be prevented by the administration of tetanus-diphtheria toxoid (Td) instead of tetanus toxoid as a booster dose.
CONCLUSION
Despite widespread immunization, sporadic cases of diphtheria still exist and there can be a shift in the age group affected in the immunized population. This can be kept in check by administering Td vaccine as booster dose every 10 years or as required. Microbiological confirmation in case of clinical suspicion and immediate infection control measures can help in preventing an outbreak.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Resurgence of diphtheria in North Kerala, India, 2016: Laboratory supported case-based surveillance outcomes. Front Public Health. 2017;5:218.
- [CrossRef] [PubMed] [Google Scholar]
- Bloodstream infection caused by nontoxigenic Corynebacterium diphtheriae in an immunocompromised host in the United States. J Clin Microbiol. 2012;50:2170-2.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.who.int/publications/m/item/vaccine-preventable-diseases-surveillance-standards-diphtheria [Last accessed on 2023 Mar 04]
- Diphtheria. United States: Centers for Disease Control and Prevention; Available from: https://www.cdc.gov/diphtheria/about/prevention.html [Last accessed on 2023 Mar 04]
- [Google Scholar]
- Epidemiology of diphtheria in India, 1996-2016: Implications for prevention and control. Am J Trop Med Hyg. 2017;97:313-8.
- [CrossRef] [PubMed] [Google Scholar]
- Available from: https://www.cdc.gov/diphtheria/clinicians.html [Last accessed on 2023 Mar 04]
- Resurgence of diphtheria in rural areas of North Karnataka, India. Indian J Med Microbiol. 2017;35:247-51.
- [CrossRef] [PubMed] [Google Scholar]
- Recent outbreaks of diphtheria in Dibrugarh District, Assam, India. J Clin Diagn Res. 2016;10:DR01-3.
- [CrossRef] [PubMed] [Google Scholar]
- Re-emergence of diphtheria in Malappuram District, North Kerala, India. J Acad Clin Microbiol. 2018;20:37-9.
- [CrossRef] [Google Scholar]




