
Translate this page into:
Pink and white esthetic management of peg laterals – A case report
*Corresponding author: R. Seshan Rakkesh, Department of Conservative Dentistry and Endodontics, Sri Ramachandra Dental College and Hospital, Chennai, Tamil Nadu, India. seshan.rakkesh@sriramachandra.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Navayath M, Ramesh SR, Kalaiselvam R, Rajendran MR. Pink and white esthetic management of peg laterals – A case report. Sri Ramachandra J Health Sci. 2023;3:68-71. doi: 10.25259/SRJHS_29_2023
Abstract
Introduction:
A set of evenly shaped anterior teeth and good soft tissue (pink) to tooth (white) ratio makes a harmonious and pleasing smile. Peg lateral is one of the most common morphological anomalies in the Indian population with an incidence of 9.14% has been recorded.
Case Summary:
Minimally invasive bonded restorations were planned to transform the smile of a 36-year-old male patient, who presented with peg laterals causing a dissatisfied smile. A pleasing smile was achieved with smile designing, use of LASERs and ceramic veneers. Ceramics veneers have a 20 year long tested clinical survival rate of 91.73%.
Conclusion:
Minimal preparation ceramic veneers can be the ideal conservative management for diastema caused due to morphological aberrations when case selection is done meticulously.
Keywords
LASER
Lithium disilicate
Peg lateral
Veneer

INTRODUCTION
A diastema is “the space between two or more adjacent teeth.” Diastemas or spacing maybe caused due to a variety of etiology including oral habits, soft tissue imbalances, physical impediments, dental anomalies, and/or dental/ skeletal disharmonies.[1] Both soft tissue (including gingival contour and margins) and hard tissue (tooth morphology) components are important criteria for achieving a pleasing esthetic smile.
Various authors have shown that maxillary lateral incisors play a major role in anterior smile esthetics.[2] However, they are known to be commonly missing or morphologically aberrant in human dentition with an incidence of 23%.[3] Grahnén defined a peg shaped tooth as “one where the incisal mesiodistal width is lesser than the cervical width.”[4] A peg shaped lateral incisor commonly looks conical with convergent mesial and distal edges.
Due to minimal surface area in a peg lateral, the challenge arises when the dental professional attempts to aesthetically and functionally rehabilitate such a condition. Thus, the treatment modalities must include proper management of the soft tissues (pink esthetics) and hard tissues to obtain a pleasing result. The treatment usually becomes multidisciplinary due to the need to modify soft tissues. The cosmetic needs of today’s society demand highly esthetic restorations and minimally invasive techniques. Various treatment options include all ceramic crowns, direct or indirect composite veneers, and ceramic veneers.[5]
This clinical case report presents a patient with bilateral maxillary peg laterals who was rehabilitated using a multi technique approach of LASER gingivoplasty followed by ceramic veneers to close the diastemas.
CASE REPORT
A 37-year-old male patient reported to the Department of Conservative Dentistry and Endodontics, Sri Ramachandra Dental College and Hospital with the complaint of spacing between his upper front teeth. This led to his dissatisfaction with his smile and inability to converse confidently with peers. At his first visit, pre-operative photographs were taken to analyze the pink (gingiva) and white (teeth) elements [Figure 1]. Further, study casts were made to evaluate his smile in three dimensions.

- Pre-operative images.
On examination, there were bilaterally present peg laterals and diastema was due to the same. On further examination and analysis of pre-operative photographs, it was seen that the gingival zenith (highest gingival margin position) in the left quadrant was higher than the right quadrant. Moreover, the gingival zenith in the left central incisor was more distally placed giving the illusion of a mesially tilted tooth [Figure 2]. Thus, pink esthetics were corrected first.
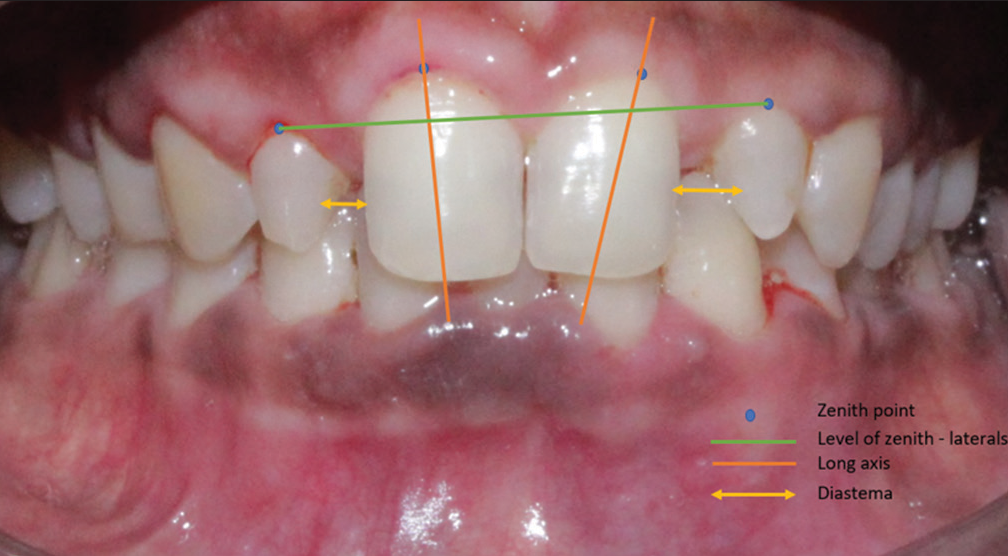
- Pre-operative smile analysis.
Pink esthetics – LASER gingivoplasty
Gingivoplasty was done with Biolase Diode LASER (EpicX, BIOLASE, Inc., Foothill Ranch, CA, USA) at the average power setting of 0.5W in a pulsed mode. The Diode Laser was used in a sweeping motion across the gingival margin in a contact mode [Figure 3a-d]. Around 0.4–0.5 mm gingival tissue was removed from the cervical region of the right maxillary incisor. The gingival contouring with respect to other teeth was minimal and only involved reshaping the free margin. At 5 day follow-up, the gingiva appeared completely matured.

- (a) Laser gingivoplasty and post gingivoplasty images – (b) end on, (c) right lateral, (d) left lateral views.
White esthetics – ceramics
A wax up of study cast using soft wax [Figure 4a] served as a guide to prepare a putty index for the intraoral mock up [Figure 4b] using Bis acrylates (Structur 2 SC, Voco, Cuxhaven, Germany).
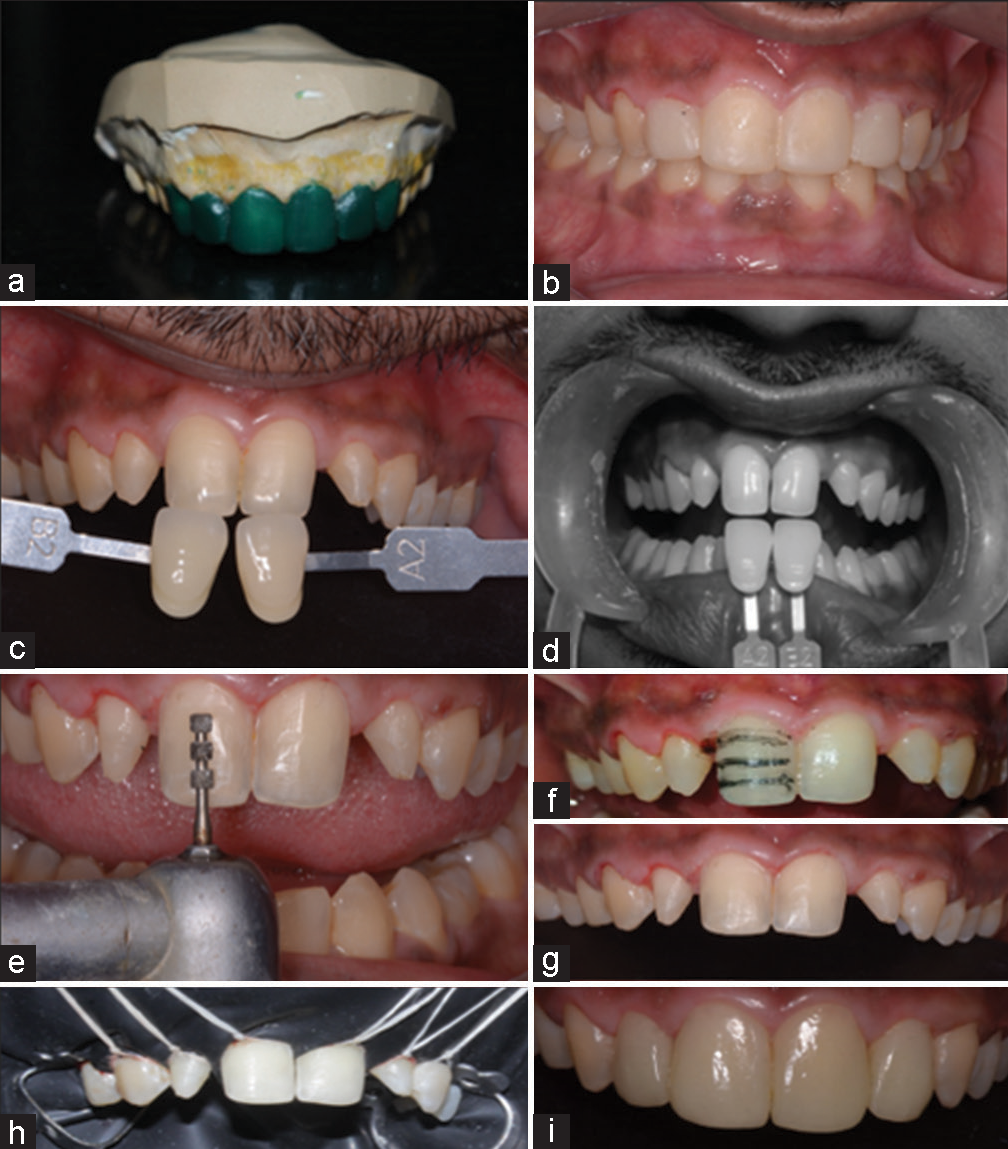
- (a) Wax up of master cast and (b) mock up with bis acryl intra oral, (c and d) Shade matching in normal and monochromatic views, (e and f) depth marking for tooth preparation, (g) tooth preparation lateral and central incisors, (h) isolation of teeth with rubber dam, (i) post cementation.
Before preparation, shade matching was done under normal and monochromatic light. Shade A2 matched closest to the dentition [Figure 4c and d] (Shade Guide: VITA classical A1-D4, VITA Zahnfabrik, Bad Säckingen, Germany). Depth grooves of 0.5 mm were marked using DM-305 (Mani, Tochigi, Japan) [Figure 4e and f]. A tapered rounded end fine diamond was used for final preparation TC-16 (Mani, Tochigi, Japan). Tooth preparation was done with incisal butt joint and ended at the transitional line angles [Figure 4g]. Master impressions were taken in elastomeric impression material of the prepared teeth (Elite HD+, Zhermack, Badia Polesine, RO, Italy).
Lithium disilicate ingots were pressed to construct the restorations. (E. max LS2, Ivoclar vivadent, Zurich, Switzerland). Before final cementation, the veneers were evaluated for adaptation, fit and color of adhesive cement using a clear try in paste. After cleaning the try in paste from the veneers, rubber dam isolation of the teeth was done [Figure 4h]. Surface treatment of intaglio surface of veneer was done as follows: first, 9.8% buffered hydrofluoric acid was used for 90 s. Followed by washing, drying and application of universal single component bonding agent (Monobond N, Ivoclar vivadent, Zurich, Switzerland) for 1 min. The tooth substrate was treated as follows: etching with 37% phosphoric acid for 30 s, washing and air drying and application of light curing resin adhesive (Variolink N LC, Ivoclar vivadent, Zurich, Switzerland). Then, the adhesive loaded veneer was positioned with Optrastick (Ivoclar vivadent, Zurich, Switzerland), followed by tack curing for 10 s. After removal of excess cement, the veneers were cured for 40 s each [Figure 4i]. Final occlusal adjustment was done and post glazing polishing was performed with rubber polishing points after removing the rubber dam. The outcome is shown in the intraoral [Figure 5] and extraoral [Figure 6] photographs.

- Post operative (above) compared to pre operative (below).

- Post-operative.
DISCUSSION
In a meta-analysis performed in 2013, prevalence of peg shaped maxillary permanent lateral incisors was 1.8% worldwide and 3.2% in Asia.[6] A study conducted among the population of Chennai, the occurrence of peg lateral was found to be 0.9%.[7] This accounts to 1 in every 100 people having either one or two peg laterals. Thus, it is imperative for dental professionals to be aware of the various treatment modalities that are available for such teeth.
In the case discussed, we have chosen to perform gingivoplasty using soft tissue diode LASER. The advantages of using LASER are far superior including minimal discomfort, no bleeding and reduced chances of swelling or tissue reactions. For the operator, the procedure is predictable, quick, and precise.[8]
Dental reanatomization can be performed using direct composites, indirect composites and ceramics.[9] Ceramics provide high gloss, long-term color stability, resistance to wear, and excellent biocompatibility. They also show low plaque accumulation and better periodontal health.[10] Moreover, silicone oxide based ceramics have a high amount of glass phase. This allows for good transparency and hence a “chameleon effect” with these ceramics; making them highly esthetic.[10]
Magne and Belser have shown that a higher loss of facial enamel causes more flexing of the tooth leading to marginal leakage and discoloration. However, glass ceramics are able to restitute the mechanical properties that are lost due to reduction of enamel and their tangential stress recovery is similar to natural tooth making the restoration biomimetic.[11] Further, pretreatment of glass ceramic with hydrofluoric acid reduces the porosities, increases the crystal size and surface area, thereby reducing the crack propagation and increasing the bond strength respectively.[10] The ionic bond achieved using organofunctional silanes as coupling molecules (Monobond N) with the adhesive resin further enhances the bond strength.
The minimal all enamel preparation in this case provided the most durable micromechanical bond with the natural tooth. This has been also demonstrated by AlJazairy in 2021, in a 20 year long clinical study which showed a 91.73% survival rate of ceramic veneers bonded to enamel.[12] Total etch technique was employed as the preparation was intra enamel.
The patient has been followed up for 6 months and excellent gingival health and superior esthetics were recorded at his last follow-up.
CONCLUSION
Ceramic veneers are an excellent option for rehabilitation of a patient with morphologically aberrant teeth. They act as perfect enamel replacements, and thus are biomimetic. A detailed planning, correct selection of dental materials and good communication with the technician contributes to a harmonious and functional smile that satisfies both patient and professional.
Ethical approval
The research/study complied with the Helsinki Declaration of 1964.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Use of artificial intelligence (AI)-assisted technology for manuscript preparation
The author(s) confirms that there was no use of artificial intelligence (AI)-assisted technology for assisting in the writing or editing of the manuscript and no images were manipulated using AI.
Financial support and sponsorship
Nil.
References
- The management of spacing in the maxillary incisor region. Br J Orthod. 1978;5:35-9.
- [CrossRef] [PubMed] [Google Scholar]
- A review of hypodontia: Classification, prevalence, etiology, associated anomalies, clinical implications and treatment options. World J Dent. 2013;4:117-25.
- [CrossRef] [Google Scholar]
- Hypodontia in the permanent dentition a clinical and genetic investigation. Odont Rev. 1956;7:1-100.
- [Google Scholar]
- Sturdevant's Art and Science of Operative Dentistry (7th ed). Netherlands: Elsevier; 2019.
- [Google Scholar]
- Prevalence of peg-shaped maxillary permanent lateral incisors: A meta-analysis. Am J Orthod Dentofac Orthop. 2013;144:97-109.
- [CrossRef] [PubMed] [Google Scholar]
- Prevalence of peg lateral among dental outpatients. J Pharm Negat Results. 2022;13:1182-8.
- [CrossRef] [Google Scholar]
- Diode laser versus scalpel in the treatment of hereditary gingival fibromatosis in a 6-year old boy. Clin Pract. 2016;6:895.
- [CrossRef] [PubMed] [Google Scholar]
- Case report esthetic rehabilitation of the smile with no-prep porcelain laminates and partial veneers. Case Rep Dent. 2015;2015:452765.
- [CrossRef] [PubMed] [Google Scholar]
- Biomimetic Restorative Dentistry. Vol 1. United Kingdom: Quintessence Pub Co.; 2022.
- [Google Scholar]
- Survival rates for porcelain laminate veneers: A systematic review. Eur J Dent. 2021;15:360-8.
- [CrossRef] [PubMed] [Google Scholar]




