
Translate this page into:
Human psychophysiology in Antarctica
*Corresponding author: Mohit Nirwan, CCRYN Collaborative Center for Mind-Body Intervention through Yoga, Raipur, Chhattisgarh, India. mohitnirvan123@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Nirwan M. Human psychophysiology in Antarctica. Sri Ramachandra J Health Sci 2022;2:12-8.
Abstract
Antarctica is a natural laboratory for scientists and an adventure destination for tourists. It has challenging yet beautiful landscape. Due to extreme environment and isolation, wintering over in Antarctica is still challenging, even with advancement in accommodations. Polar scientists have focused on the aspects of Antarctica according to their specialty. For example, psychologists have highlighted polar psychology; likewise, physiologists and other allied human biologists have pointed-out to biochemistry, immunology, and stress biology. A researcher new to Antarctica gets confused to encounter diverse literature of different domains. These reasons require a review on the scientific aspects of wintering-over in Antarctica to enlighten first time readers. Journal articles from PubMed and Google Scholar (up to 2021) were searched with the search terms “Antarctica,” in combination with the words “human physiology” and “human psychology”. Vivid direct quotes of early explorers of the heroic age of polar expeditions are described and 53 articles were finally selected. The human psychophysiology points of discussion in this narrative review are geomagnetism, circadian rhythm, immunity, hypoxia, bone metabolic changes, acute mountain sickness, and stress biology concerning extended stay in Antarctica.
Keywords
Polar
Physiology
Psychology
Wintering-over
Human isolation

INTRODUCTION
Antarctica is the most isolated continent on earth. It has recorded extreme climates due to cold, wind, photoperiod, terrain, geomagnetism, and dry air. Countries keep their respective research bases in Antarctica and send rotating teams to live there generally for 3 or 14 months. People can reach Antarctica via airplane or ship. The arrival in Antarctic waters is a pleasure because of the scenic views, followed by exhausting labor for days as the ship/airline is unloaded and station supplies are replenished. No ship can sail in the Antarctic waters during the austral winter period from March to October because of thick ice mass. Air routes are also impossible due to blizzards and darkness. There can be no resupply until next year leading to lack of fresh vegetables and milk.
This narrative review facilitates a reader new to Antarctica on the aspects of wintering-over there. Vivid direct quotes of early explorers of the heroic age of polar expeditions are described. The geomagnetism, circadian rhythm, immunity, hypoxia, bone metabolic changes, acute mountain sickness (AMS), and stress biology concerning extended stay in Antarctica are discussed.
MATERIAL AND METHODS
Journal articles from PubMed and Google Scholar (up to 2021) were searched with the search terms “Antarctica,” in combination with the words “human physiology” and “human psychology”. The lists of articles recognized by this search hit were scrutinized [Figure 1]. The literature search focused on psychological, physiological, immunological and biochemical dimensions of human’s wintering over Antarctica. However, critical publications that generalized on aspects common to the Arctic and other isolated and extreme confined environments (ICE) are also included in the study. Various articles known earlier are also included.
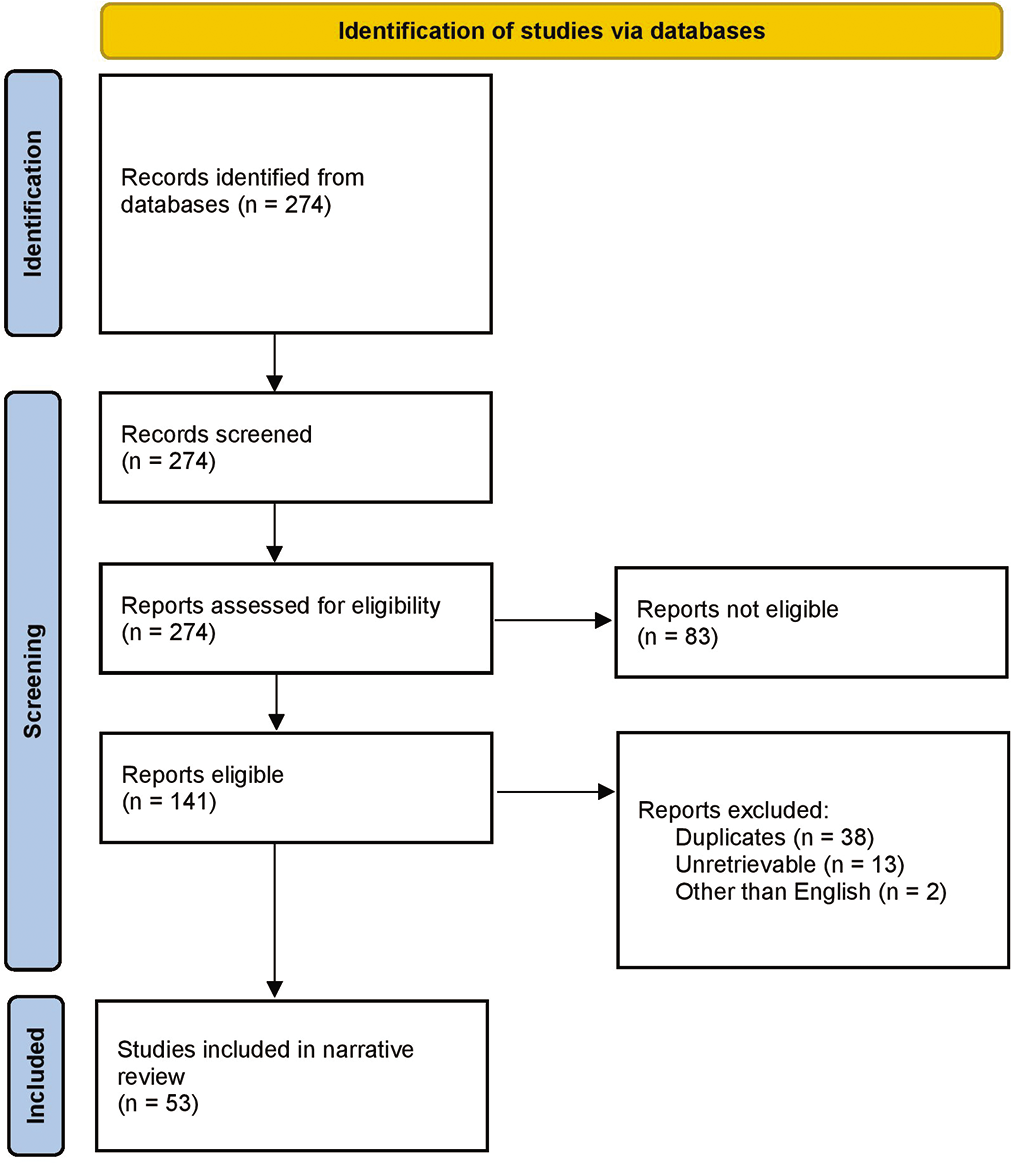
- A flowdiagram depicting the selection of studies for the narrative review.
Psychology in Antarctica
The first thing that happens on reaching Antarctica is the devastation of sleep. Antarctic arrivals of the expedition teams are conducted in austral summer (November–February); on reaching the continent, illumination with constant bright sunlight disrupts the biological clock. The individual also faces constant darkness during the austral winters. This change in photoperiod starts a constellation of psychological problems in an individual.
Polar station settings are stressful in terms of boredom, limited supplies and equipment. Confinement in the Antarctic is not because of the small living space but due to the inability to leave the station and the group.[1] There is a complete physical separation from family and friends for months. Harrison and Connors stated that, “Typically, mood and morale reach nadir somewhere between the one-half and two-thirds mark of the mission,” popularly known as the third-quarter phenomenon. A medical doctor in the Belgian expedition (1897–9) said that, “The curtain of blackness which has fallen over the outer world of icy desolation has also descended upon the inner world of souls…. men are sitting about sad and dejected, lost in dreams of melancholy…. all efforts to infuse bright hopes fail”(Cook, 1900/1980:282). On Scott’s second expedition, Debenham quoted it as, “the scenery has lost much of its beauty to us, the auroras are cheap and the cold rather colder.”[1]
There are three broad stages of common human reaction in an ICE set. The first stage is heightened anxiety when the individual arrives in Antarctica or any ICE. The second stage is the ensuing depression and settling down to the routine forced. Near completion of the expedition, the third stage that can be detrimental for the individual and the team is emotional outbursts, aggressiveness, and rowdy behavior.[2] Sometimes, adverse human reactions and consequences have been overestimated in ICE environments.[3] Participants also encounter favorable experiences and may positively transform their personality and do better in their professional and personal lives after returning to civilization. This change in one’s orientation is recognized as “salutogenesis,”[4] that is a positive attitude towards life and increased self-confidence. Salutogenic behavior may arise due to accomplishment after adjusting to a new and unique environment. It can result from a sense of heroism, bravery, self-sacrifice, and conquest.[5,6]
Social erosion has been frequently reported in polar expeditions. One of the reasons is the lack of will for clear communication among the team members. The team leaders’ efficiency and sensitivity to the needs and welfare of the team members also play a pivotal role.[7-9] The team leaders’ governance practices affect team members’ communication, output, and morale. The crew under strict leaders has less open communication and work output than the leaders, which fosters a relaxed and harmonious work environment.[10] Differences in occupations among the team members can cause friction and conflicts because Antarctic teams are composed of scientific and other coordinators. The scientists have a specific research task, and they may not quickly “mold” to the station duties as good as the coordination personnel and contribute to the “role stress.” An Antarctic team consisting of team members with average rates of extraversion-introversion and low neuroticism and psychoticism does well.[11]
Team members overwintering in Antarctica also come across “intellectual inertia” in which decreased intellectual ability was noticed to any added tasks or projects given during near completion of the expedition. It is characteristic of diminished memory and concentration. The phenomenon was best described because of a lack of sensory inputs and relatively “sameness” encountered by the team members overwintering.[12]
The modern Antarctic stations are equipped with the internet; this feature has positive and negative effects on psychological well-being. Personnel can stay connected with their family and friends, thus reducing social isolation. However, at the same time, if any problem occurs in their social circle, then they feel helpless.[5]
The main challenge faced by the expedition team during austral winter by early explorers is described [Figure 2] as the qualities of an explorer as “optimistic; patient physically fit; the man with a cheerful disposition and ready laugh is a bright sun to his companions and a great help to the leader of the expedition.”[1] Shackleton’s statement seems factual following an excerpt from the diary of his expedition team member Frank Wild: “several times I fell into crevasses, as everyone did. While hanging in the harness I prayed that the rope would break so that I would have a nice long rest.”[13]
- Working in Antarctica can bring favorable behavioral modifications like a sense of achievement and higher self-confidence later in life. It is also associated with a constellation of psychological issues.
Physiology in Antarctica
Physical stress is caused due to working in rough terrain often covered with snow. It tremendously increases the load and maybe tolerated by the individuals having lower baseline change in maximal oxygen consumption (VO2MAX) than those with already higher VO2MAX.[14] Injuries are the most common morbidity among Antarctic expedition teams.[15] Working in icy conditions can bring musculoskeletal disorders and increased chances of slips, trips, falls, and cognitive impairments, leading to a decrease in the chances of survival.
Task performance under 10°C for durations higher than 2 h can adversely affect physiological well-being.[16]
Disturbance in the normal levels of the hypothalamic-pituitary-thyroid axis has been reported in the polar sojourners.[17,18] A decrease in total and free triiodothyronine thyroid hormone with increased thyroid-stimulating hormone. This phenomenon is known as Polar T3 syndrome. The expected level of thyroid hormones is critical for keeping metabolism, cold acclimatization, and mood. The abnormal fluctuations of the thyroid hormones seriously affect the well-being of an individual in circumpolar regions. The clinical significance of the syndrome can be determined by thyroxine supplementation, and yoga has been suggested to manage polar T3 syndrome.[9,19]
Cortisol, a glucocorticoid and a stress biomarker, has increased during an Antarctic expedition. Due to the unregulated hypothalamus-pituitary-adrenal axis and sustained elevated glucocorticoid levels. Prolonged exposure to glucocorticoids can cause atrophy of the hippocampus neurons and poor memory.[20] If a strict routine is forced on the team-mates, then a disturbance in diurnal rhythms of cortisol and some symptoms of over-winter syndrome can be prevented.[21] Higher levels of plasma noradrenaline were found with higher latitude Antarctic residence.[22]
Autonomic balance and menstrual cycle
Studies in Antarctica over WOT reported sympathetic dominance among WOT.[23] Sympathetic dominance could cause hypertension, hypercortisolism, high breathing and heart rate, and poor sleep. Sympathetic overdrive can have adverse health effects.
A study reported suppression in luteinizing hormone reactivity before and during an Antarctic traverse, whereas follicle-stimulating hormone did not change during and after the expedition.[24]
Circadian rhythm and melatonin
In normal geographical conditions, the pineal secretion of melatonin occurs from late evening to early morning. Apart from external cues, the circadian rhythm depends on work habits, meal times, and social interactions. The periodicity of circadian rhythm is ~24h typically. However, it runs freely in polar and space environments with decreased stability.[25] Antarctica is a natural laboratory to study circadian rhythm omitting the 12h day-night cues. Pattyn et al., and Arendt reviewed the topic independently and concluded a delay in sleep onset and awakening and sleep fragmentation in Antarctica, including an inconclusive trend of melatonin secretion.[26,27]
Hypoxia along with extreme cold!
Antarctica has the highest average altitude among all the continents.[28] The barometric pressure in polar conditions is not equivalent to lower latitudes’ atmospheric pressure at the same altitude. The earth’s spin and cold air caused by the Ferrel cell wind belt alter the barometric pressure to be lower than what would be expected at the physical altitude of the South Pole altitude.[29] Many Antarctic stations are located near the South Pole and are at a considerable altitude above sea level. Life is more stressful in such stations than at Antarctic seashores or near sea level.
AMS can rapidly occur in individuals traveling to altitudes over 2500m. It is generally assessed by a self-reported questionnaire called as Lake Louise questionnaire.[30] The researchers found a significant reduction in blood pCO2 and, consequently, an increase in blood pH at harmful base excess in the WOT and persistently increased hemoglobin concentration during the stay.[31] Physical exertion due to extensive outdoor work in extreme cold increases AMS incidence significantly in the polar regions.[29] Using oral contraceptive pills increases the risk of developing AMS.[32] Researchers reported increased hematocrit, thrombocyte, lymphocyte, granulocytes, and monocytes while staying in the French-Italian Concordia station. They informed a significant decrease among lymphocyte subsets in the T-cell percentage, with a corresponding B-cell elevation.[33] Periodic breathing, sleep fragmentation, and other sleep disturbances are common problems encountered in the Antarctic and other hypoxic environments.[34] More than half of the Antarctic expeditioners who were uplifted to high altitude experienced symptoms of AMS.[35]
Infections and immune response
The Antarctic environment is more sterile than other continents on earth. That is why there is diminished immune responsiveness in the wintering team. The lack of environmental and human propagated antigens and extreme cold and wind induce immune latency.[36] Incidences of infections are low or absent in most expeditions. However, minor outbreaks, especially for upper respiratory infections, can occur during contact in the overlap period of the new expedition team with its predecessor team. For example, from 1956 to 2000 at Syowa station, the maximum number of common cold cases build-up in December, the month when fresh Antarctic recruits arrive.
Stress associated with wintering in Antarctica alters immune functions. Increased serum IgA and TH1 cytokines have been reported among WOT compared to their baseline levels.[37] Shirai et al., 2003, have reported a decrease in the serum levels of TNF-α, IL-6, and IL-1β and a significant increase in the natural killer T-cells during Antarctic isolation. They found that exposure to Antarctic winter induces TH1-skewed immunity in human beings. An imbalance between TH1 and TH2 immunity which can lead to immune-associated diseases.[38] No significant changes were found in secreted human leukocyte antigen-G in Antarctic expeditioners.[39]
A study reported reduction in the proliferation of PBMC to phytohemagglutinin and depressed cutaneous delayed-type hypersensitivity reactions following 120 days of Antarctic isolation.[40] Also, salivary IgA levels are low in March–May and the IgM levels low in Jan-April with peak levels in June-July.[41]
Bone metabolic changes
Seasonal changes in Vitamin D synthesis and physical activity have been associated with bone metabolism. Age also influences it, so older adults are more susceptible to these changes than younger people. Vitamin D has two main types: Vitamin D3 (cholecalciferol) and Vitamin D2 (ergocalciferol). Cholecalciferol is synthesized utilizing 7-dehydrocholesterol of the cell membranes in the skin following exposure to ultraviolet B radiation, and ergocalciferol is formed by plants and obtained from the diet. Animals can also synthesize Vitamin D3 and, therefore, be obtained in the diet. Vitamin D is metabolized in the liver to an inactive 25-hydroxyvitamin-D [25(OH)D]. Therefore, serum 25(OH) D reflects the amount of Vitamin D in the body. It is accepted that a 25(OH)D concentration <20 ng/ml reflects deficiency. The D3 form is more effective in increasing 25(OH)D levels than the D2 form. Vitamin D is a significant player in calcium homeostasis because it facilitates the body’s higher absorption of dietary calcium and phosphorus.[42]
In austral winters, it was found that serum 25(OH)D3 decreases due to significantly fewer hours of sunlight or no sunshine at all.[43] However, the decrease was found within the clinical limits indicating utilization of reserve Vitamin D stored in the liver or intake from the diet, especially fish. Another study reported a reduction in serum 25(OH)D3 in overwintering team members. Higher baseline Vitamin D serum concentrations have been suggested to overcome the deficiency.[44] Iuliano-Burns et al., 2009, reported Vitamin D deficiency in 85% of the Australian expedition team after 6 months of winter-over in Antarctica. They informed a decrease in bone mass density in the members with serum 25(OH)D levels <50 nmol/L. They advised baseline assessments of serum 25(OH)D and supplementation for those with serum 25(OH)D levels <100 nmol/L. Decline in serum 25 (OH)D below <50 nmol/L was prevented through Vitamin D supplementation in the winter-over team.[45] A decrease in the calcium content in human hair after 1 month’s stay in Antarctica has been associated with insufficient Vitamin D levels.[46] High dietary sodium intake increases renal calcium excretion and can create a negative calcium balance, contributing to bone loss. Furthermore, heavy alcohol consumption intake contributes to decreased bone density.[47]
Geomagnetism
A few researches have been conducted on the influence of geomagnetism on human physiology in polar geology. Geomagnetic force varies from 35 µT on the equator to 65 µT in circumpolar regions. The polar sojourners are bombarded with electromagnetic (EM) radiations, radiations from radionuclides such as thorium deposits in Antarctica,[48] and high-intensity solar flux and eruptions throughout the austral summer. Interestingly, the magnetic part of the EM wave has been playing a dominant role in the onset of biological effects because of its ability to penetrate the human tissue. It has been proposed that the magnetic field increases the half-life of the free radicals in a biological fluid and interacts with the plasma membrane of cells to influence the ion transport across the membrane.[49]
A common observation while living in a polar environment is the spark discharges from the skin. The ambient electric field settles on the body surface area and builds up continuously[50] until discharged while touching another person or metallic objects.
DISCUSSION
Antarctica is an excellent analog for the isolation and confinement of space missions.[38] Although not perfect, Antarctica is the closest analogy to outer space found on earth. It has an extreme cold and social isolation and thus threatening.[10]
Polar biologists insisted that the Vitamin D deficiency is due to the lack of sunlight in the winter months; however, the clothing factor was not considered. Antarctic sojourners must wear three layers of clothing having the outer layer of 100% synthetic material, windproof, and insulation: Middle and inner layer with mixed polyester and cotton clothing. It is implausible that even if there is ample sunlight available in Antarctica, there will be no Vitamin D insufficiency because UV radiation cannot penetrate enough of the skin after passing through so many layers of clothing. The author is putting up this thought because Vitamin D insufficiencies were found even in tropical countries like Brazil (Mendes et al., 2018)[51] where both the line of equator and line of Capricorn pass through supplying ample sunshine throughout the year. Furthermore, almost half of the expeditioners have been found to have <50 nmol/L of serum 25(OH)D in their baseline data before reaching Antarctica.[52]
It has been previously reported that there is a significant decrease in plasma insulin levels during austral winter. The authors have speculated that it increases heat production by increasing substrate availability through lipolysis and hepatic glucose output.[53] The author measured increased glucose levels of wintering Antarctic members during his expedition (unpublished data). It may be a vital habituation feature to the cold environment as high glucose increases blood osmolarity, which helps prevent and manage cold injuries.
The resilience trait has been a functional adaptive behavior to counter ice. However, in ice covered long-term like winter-over in Antarctica, the resilience trait needs replenishment of the personal resources, positive thoughts, and will power to combat the psychological stress. This replenishment is achieved through a “break” from the stressful situation through good-night sleep or privacy from the group[10] or through mind-body interventions like yoga.[8] However, the team’s need for privacy may be underestimated by the leaders and managers of the Antarctic expeditions.
A statistically correct number of participants are rarely achieved in any Antarctic expedition due to the limited number of people in a winter-over team. Antarctica offers only a tiny sample size for studies of hardly generalizable data, which can also differ between expeditions. Therefore, many studies or data in successive expeditions are needed to prove biological significance. Studies are summarized in [Table 1 and Figure 3].
- Antarctic terrain and extreme weather can ensue stress at physical and physiological homeostasis levels.
| Outcome of interest | Reference | Summary of key findings |
|---|---|---|
| Bone mass | [43] | No changes in bone mass; a significant decrease in 25(OH) D3 with a reduction in sunshine hours but within the normal clinical range |
| [52] | Bone mass density decreased in the expeditioners that have vitamin D insufficiency (<50 nmol/L) | |
| [45] | Decrease in 25(OH) D3 in the members who did not take Vitamin D supplements during winter-over | |
| Immunity | [37] | Increased sIgA and TH1 cytokines in the expedition team compared to their baseline values |
| [38] | A significant increase in the natural killer T-cells during Antarctic isolation; Antarctic winter induce TH1-skewed immunity | |
| [39] | No significant changes were found in secreted human leukocyte antigen-G in Antarctic expeditioners | |
| [40] | Reduction in the proliferation of PBMC to phytohemagglutinin and depressed cutaneous delayed-type hypersensitivity reactions following 120 days of Antarctic isolation | |
| [41] | Salivary IgA levels low in March–May; IgM levels low in Jan-April with peak levels in June-July | |
| [33] | Increase in the B-cell and a decrease in the T-cell during mid-winter | |
| Stress | [8,37] | Increased cortisol in the expedition team compared to their baseline values |
| [21] | No disturbance was found in the diurnal rhythm of cortisol in the over-wintering team, although sleeplessness and fatigue scores were high | |
| [9,23] | Reported sustained increased noradrenaline during the whole expedition | |
| [22] | Higher levels of plasma noradrenaline were found with higher latitude Antarctic residence | |
| [53] | Significant decrease in insulin levels of the team during Antarctic winter | |
| [46] | Decrease in the levels of human hair Ca, Cu and Mg after 1-month Antarctic stay | |
| [17] | Dwindling of the serum thyroid hormones after a prolonged Antarctic stay | |
| [24] | A suppression in luteinizing hormone reactivity before and during an Antarctic traverse whereas follicle-stimulating hormone did not change during and after the expedition |
CONCLUSION
Physiologically and maybe psychologically, we are far more adapted to heat than cold.[54] Winter-over in Antarctica has been associated with psycho physiological, social, cultural, and occupational variables. Research bases in Antarctica are increasing and expanding, so more people come for work and leisure. Hence, thorough information about human behavior and psycho physiological response due to the Antarctic environment and confinement is essential for polar sojourners.
Acknowledgments
I would like to thank the Defence Institute of Physiology and Allied Sciences under the aegis of the Defence R&D Organization for facilitating my Antarctic voyage and stay.
Declaration of patient consent
Patient’s consent not required as there are no patients in this study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflict of interest.
References
- Psychology during the expeditions of the heroic age of Antarctic exploration In: Hist Psychiatry. Vol 23. 2012. p. :194-205.
- [CrossRef] [Google Scholar]
- The third-quarter phenomenon: Do people experience discomfort after stress has passed? In: From Antarctica to Outer Space. New York: Springer; 1991. p. :261-5.
- [CrossRef] [Google Scholar]
- The environmental psychology of of capsule habitats. Annu Rev Psychol. 2000;51:227-53.
- [CrossRef] [PubMed] [Google Scholar]
- The salutogenic model as a theory to guide health promotion 1. Health Promot Int. 1996;11:11-8.
- [CrossRef] [Google Scholar]
- Human performance in polar environments. J Environ Psychol. 2011;31:353-60.
- [CrossRef] [Google Scholar]
- Psychological effects of polar expeditions In: Lancet. Vol 371. 2008. p. :153-63.
- [CrossRef] [Google Scholar]
- Affective, social, and cognitive outcomes during a 1-year wintering in concordia. Environ Behav. 2016;48:1073-91.
- [CrossRef] [Google Scholar]
- Improvement in resilience and stress-related blood markers following ten months yoga practice in Antarctica. J Complement Integr Med. 2020;18:201-7.
- [CrossRef] [PubMed] [Google Scholar]
- Yoga intervention as a potential countermeasure for polar T3 Syndrome. Def Life Sci J. 2019;4:163-9.
- [CrossRef] [Google Scholar]
- The human experience in antarctica: Applications to life in space. Behav Sci. 1989;34:253-71.
- [CrossRef] [PubMed] [Google Scholar]
- Main features of expeditioners personality traits in Antarctic conditions In: Ment Health Glob Chall. Vol 4. 2021. p. :1.
- [CrossRef] [Google Scholar]
- Some Psychological aspects of Isolated Antarctic Living In: 116th Annual Meeting of the American Psychiatric Association 1960. p. :323-5.
- [CrossRef] [PubMed] [Google Scholar]
- Psychiatric illness and suicide in the heroic age of Antarctic exploration. Hist Psychiatry. 2012;23(Pt 2):206-15.
- [CrossRef] [PubMed] [Google Scholar]
- The changes in maximal oxygen uptake (VO2MAX) induced by physical exertion during an Antarctic expedition depend on the initial VO2MAX of the individuals: A case study of the Brazilian expedition In: Int J Circumpolar Health. Vol 77. 2018. p. :1521244.
- [CrossRef] [PubMed] [Google Scholar]
- Morbidity pattern of the 27th Indian scientific expedition to antarctica In: Wilderness Environ Med. Vol 23. 2012. p. :231-8.e2.
- [CrossRef] [PubMed] [Google Scholar]
- Task-dependent cold stress during expeditions in antarctic environments In: Int J Circumpolar Health. Vol 76. 2017. p. :1379306.
- [CrossRef] [PubMed] [Google Scholar]
- Alterations in the hypothalamic-pituitary-thyroid axis after prolonged residence in antarctica. Clin Endocrinol (Oxf). 1986;25:55-65.
- [CrossRef] [PubMed] [Google Scholar]
- Circannual pattern of hypothalamic-pituitary-thyroid (HPT) function and mood during extended antarctic residence. Psychoneuroendocrinology. 2001;26:421-31.
- [CrossRef] [Google Scholar]
- Impairment in cognitive and exercise performance during prolonged antarctic residence: Effect of thyroxine supplementation the polar triiodothyronine syndrome. J Clin Endocrinol Metab. 2001;86:110-6.
- [CrossRef] [PubMed] [Google Scholar]
- Increase in urinary cortisol excretion and memory declines: MacArthur studies of successful aging. J Clin Endocrinol Metab. 1997;82:2458-65.
- [CrossRef] [PubMed] [Google Scholar]
- Diurnal rhythm in British Antarctic personnel. Rural Remote Health. 2010;10:1351.
- [CrossRef] [PubMed] [Google Scholar]
- Environmental influences on hypothalamic-pituitary-thyroid function and behavior in Antarctica. Physiol Behav. 2007;92:790-9.
- [CrossRef] [PubMed] [Google Scholar]
- Autonomic nervous system and adrenal response to cold in man at Antarctica. Wilderness Environ Med. 2005;16:81-91.
- [CrossRef] [PubMed] [Google Scholar]
- Female reproductive, adrenal, and metabolic changes during an antarctic traverse. Med Sci Sports Exerc. 2019;51:556-67.
- [CrossRef] [PubMed] [Google Scholar]
- Free-running rhythms of melatonin, cortisol, electrolytes, and sleep in humans in Antarctica. Am J Physiol. 1991;260:R1137-44.
- [CrossRef] [PubMed] [Google Scholar]
- Sleep during an Antarctic summer expedition: New light on 'polar insomnia In: J Appl Physiol. Vol 122. 2017. p. :788-94.
- [CrossRef] [PubMed] [Google Scholar]
- Biological rhythms during residence in polar regions. Chronobiol Int. 2012;29:379-94.
- [CrossRef] [PubMed] [Google Scholar]
- Psychological changes arising from an Antarctic stay: Systematic overview. Estud Psicol. 2013;30:415-23.
- [CrossRef] [Google Scholar]
- Relationship of activity patterns to acute mountain sickness in south pole workers. Int J Sports Med. 2019;40:440-6.
- [CrossRef] [PubMed] [Google Scholar]
- The 2018 lake louise acute mountain sickness score. High Alt Med Biol. 2018;19:4-6.
- [CrossRef] [PubMed] [Google Scholar]
- Lack of acclimatization to chronic hypoxia in humans in the Antarctica. Sci Rep. 2017;7:18090.
- [CrossRef] [PubMed] [Google Scholar]
- Oral contraceptive use and acute mountain sickness in south pole workers. Aviat Space Environ Med. 2013;84:1166-71.
- [CrossRef] [PubMed] [Google Scholar]
- Immune sensitization during 1 year in the Antarctic high-altitude concordia environment. Allergy Eur J Allergy Clin Immunol. 2019;74:64-77.
- [CrossRef] [PubMed] [Google Scholar]
- Altitude and Seasonality Impact on Sleep in Antarctica. Aerosp Med Hum Perform. 2015;86:392-6.
- [CrossRef] [PubMed] [Google Scholar]
- Sleep disordered breathing and acute mountain sickness in workers rapidly transported to the South Pole (2835 m) Respir Physiol Neurobiol. 2015;210:38-43.
- [CrossRef] [PubMed] [Google Scholar]
- Wintering in Antarctica: Impact on immune response of indian expeditioners In: Neuroimmunomodulation. Vol 19. 2012. p. :327-33.
- [CrossRef] [PubMed] [Google Scholar]
- TH1-biased immunity induced by exposure to Antarctic winter. J Allergy Clin Immunol. 2003;111:1353-60.
- [CrossRef] [PubMed] [Google Scholar]
- Effect of extreme conditions of antarctica on human leukocyte antigen-G in Indian expeditioners In: Indian J Med Res. Vol 140. 2014. p. :520-3.
- [Google Scholar]
- Antarctic isolation: Immune and viral studies. Immunol Cell Biol. 1997;75:275-83.
- [CrossRef] [PubMed] [Google Scholar]
- Trends in mucosal immunity in antarctica during six Australian winter expeditions In: Immunol Cell Biol. Vol 80. 2002. p. :382-90.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D: Bone and beyond, rationale and recommendations for supplementation. Am J Med. 2009;122:793-802.
- [CrossRef] [PubMed] [Google Scholar]
- Bone metabolic changes in antarctic wintering team members. Bone. 1999;24:145-50.
- [CrossRef] [Google Scholar]
- Changes of 25-OH-Vitamin D during overwintering at the German antarctic stations neumayer II and III. PLoS One. 2015;10:1-18.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D supplementation during Antarctic winter. Am J Clin Nutr. 2009;89:1092-8.
- [CrossRef] [PubMed] [Google Scholar]
- Variations in the level of some trace elements in hair of participants in the Italian expeditions in Antarctica In: J Environ Monit. Vol 7. 2005. p. :1331-4.
- [CrossRef] [PubMed] [Google Scholar]
- Dietary intakes of expeditioners during prolonged sunlight deprivation in polar environments do not support bone health In: Int J Circumpolar Health. Vol 74. 2015. p. :27965.
- [CrossRef] [PubMed] [Google Scholar]
- Measurements of background radiation levels around Indian station Bharati, during 33rd Indian scientific expedition to Antarctica In: J Environ Radioact. Vol 167. 2017. p. :54-61.
- [CrossRef] [PubMed] [Google Scholar]
- Mechanisms of geomagnetic field influence on gene expression using influenza as a model system: Basics of physical epidemiology. Int J Environx. Res Public Health. 2010;7:938-65.
- [CrossRef] [PubMed] [Google Scholar]
- Electromagnetic effects from cell biology to medicine. Prog Histochem Cytochem. 2009;43:177-264.
- [CrossRef] [PubMed] [Google Scholar]
- Vitamin D status in the tropics: Is sunlight exposure the main determinant? Nutr Bull. 2018;43:428-34.
- [CrossRef] [Google Scholar]
- Skeletal and hormonal responses to sunlight deprivation in Antarctic expeditioners In: Osteoporos Int. Vol 20. 2009. p. :1523-8.
- [CrossRef] [PubMed] [Google Scholar]
- Plasma insulin and growth hormone during antarctic residence. Jpn J Physiol. 1998;48:167-9.
- [CrossRef] [PubMed] [Google Scholar]
- 100 years since scott reached the pole: A century of learning about the physiological demands of Antarctica. Physiol Rev. 2012;92:521-36.
- [CrossRef] [PubMed] [Google Scholar]




