
Translate this page into:
Comparison of orbital volume measured using computed tomography and fluid displacement: A comparative study using dry skull
*Corresponding author: Jayakumar Naveenkumar, Department of Oral and Maxillofacial Surgery, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. naveenkumarj@sriramachandra.edu.in
-
Received: ,
Accepted: ,
How to cite this article: Suresh S, Deepak C, Naveenkumar J. Comparison of orbital volume measured using computed tomography and fluid displacement: A comparative study using dry skull. Sri Ramachandra J Health Sci 2022;2:56-60.
Abstract
Objectives:
The purpose of the study was as follows: (1) To compare orbital volume calculated using computed tomography (CT) scans with real-time measurements. (2) To evaluate if the orbital volume of the adjacent orbit can be taken as a tool of comparison for orbital volume correction in orbital fractures.
Materials and Methods:
A prospective study was conducted on 30 orbital cavities with intact orbital walls. The foramina and fissures were sealed using molding wax. Alginate impressions of the orbital cavity were taken to determine the orbital volume using the Archimedes principle. GE light speed 64 slices CT scanner was used to scan the orbits with 0.8 mm sections. Orbital volume was calculated using the CT software GE ADW 4.5 workstation.
Results:
The comparison of CT measurement and Archimedes principle measurement shows a mean and standard error of 0.2333 mm and 0.09794, respectively, on the right orbits and a mean and standard error of 0.10011 mm and 0.0981, respectively, on the left orbits.
The comparison of the right and left orbits shows a mean and standard error of 0.4067 mm and 0.2771 mm, respectively, using the Archimedes principle and a mean and standard error of 0.3300 mm and 0.2775, respectively, using CT scans.
Conclusion:
It was found that the difference in orbital volume between CT and real-time measurement is very negligible. The study shows that CT is a reliable tool for the orbital volume measurement and the adjacent orbit can be taken as a comparative tool for the orbital volume corrections.
Keywords
Orbital volume
Computed tomography
Alginate

INTRODUCTION
Orbit is a pear-shaped bony cavity which is ideally formed by contribution of seven craniofacial bones. It is lined by periosteum which is densely adherent to bone, extending from the orbital rim to optic canal covering the orbital fissures. The bony plates of orbital cavity are thin, especially the floor and medial wall, making it very fragile to maxillofacial impacts. About 40% of maxillofacial injuries (most commonly midface) involves orbital bones.[1,2] The injuries may vary from a simple blowout fracture to a complex bony disruption like in comminuted or Panfacial fracture where bone displacement is very common.[3,4] Following these injuries, the functional and esthetic impairment will be evident and major contributing factor being orbital volume alterations.
Volumetric alteration of the orbit is mostly due to herniation of orbital components into adjacent spaces (most commonly maxillary antrum) following fractures of orbital walls. This herniation leads to enophthalmos. Enophthalmos mostly is accompanied by functional impairment such as diplopia, restricted eye movements, and disturbance in visual acuity due to entrapment of herniated orbital contents between the bony fragments.[5,6] The dividing line between surgical and non-surgical management would be volume of herniated contents, associated functional and esthetic impairments, and fractured site.[7,8] Volume estimation and fracture location are confirmed using a computed tomography (CT) which makes it a very important tool in treatment planning. The other most important tool in restoring orbital volume is comparing lost volume/volume alteration with that of the adjacent orbit. Hence, we conducted a study with dry skull models with two main objectives.
To study if CT was a reliable tool for the estimation of the orbital volume
To study if orbits of same skull could be used as a comparative tool for restoring the orbital volume.
MATERIAL AND METHODS
A prospective study was conducted in 15 human dry skulls (30 orbital cavities). The study was conducted in the department of oral and maxillofacial surgery. Ethical approval was obtained from the University Ethical Committee. The inclusion criteria applied were adult human skulls with bilateral intact orbital walls, orbital rim, fissures, and foramina. The exclusion criteria applied were pediatric skulls, damaged orbit, irregular/undefined rims, and boundaries. The skulls with unilaterally intact orbits were also excluded from the study.
Anatomical landmarks
The highest point on supraorbital rim was taken as the superior boundary and the highest point on the infraorbital rim was taken as the inferior boundary. The mediolateral extent is from the anterior lacrimal crest to the frontozygomatic suture. Posterior boundary ends at the optic foramen.
All the foramina, fissures, and canal were sealed [Figure 1] with molding wax as it can be better molded to suit the anatomy and it has a better adherence to the bone without dislodging and does not cause any damage to the anatomy of the bone.

- Foramina and fissures sealed.
Archimedes principle
Archimedes’ principle is a physical law of buoyancy, discovered by the Greek mathematician, and inventor Archimedes, stating that anybody completely or partially submerged in a fluid at rest is acted on by an upward or buoyant force. The volume of displaced fluid is equivalent to that of the volume of an object fully immersed in a fluid.
This basic law of physics was taken to measure the real-time volume of the orbit.
CT scan
GE Light speed 64 slices (120 kv, 229 mA) CT scanner was used to take the CT measurements of the skulls. The thickness of the axial, coronal and sagittal sections was 0.8 mm and, hence, there were a better precision and coverage of the orbital cavity. DICOM services were used to import images for further analysis and processing.
Technique
After sealing foramina and fissures of orbital cavity such as mentioned before, cavity was filled with alginate impression material [Figure 2] keeping the above-mentioned anatomical landmarks as the extents. As soon as the impression material sets, the skulls were subjected to CT scan [Figure 3]. Once CT scan was taken, impression was removed from the cavity without distortion. Immediately after, real-time volume measurement was done using the Archimedes principle to avoid distortion. A calibrated beaker was filled with water and the level of the water was measured. The mold was then dropped carefully into the beaker and the raise in the water level was measured using a pipette for accuracy. Later, the CT volume of the orbit was measured using the workstation after transferring the images using DICOM services. The cursor was used for the segmentation of the radio opaque alginate material. Summation of segments was done using software and volume of orbits was measured.

- Alginate filled in the orbit.

- Computed tomography scan of skull model.
Ethical statement
Institutional ethical committee approval was obtained (Ref: CSP/16/AUG/50/228, dated October 30, 2017.
RESULTS
The real-time volume and the CT scan volumes of 30 orbits (15 skulls) were measured [Table 1]. The results obtained were then assessed. The comparison of orbital volume, both real time and CT scan, was done to compare right and left orbits of same skull and also the CT scan values were compared with that of the real time volume.
| Skull | CT right | FD right | CT left | FD left |
|---|---|---|---|---|
| Skull 1 | 26.5 | 26.6 | 26.9 | 26.7 |
| Skull 2 | 27.05 | 26.9 | 25.2 | 24.5 |
| Skull 3 | 27.8 | 27.5 | 25.3 | 25 |
| Skull 4 | 24.6 | 24.5 | 25.8 | 26 |
| Skull 5 | 25.4 | 25.9 | 25.5 | 25.3 |
| Skull 6 | 25.2 | 24.7 | 24.6 | 24.3 |
| Skull 7 | 26.9 | 26.9 | 28 | 27.2 |
| Skull 8 | 28 | 27.5 | 27 | 26.9 |
| Skull 9 | 27.9 | 28 | 27.7 | 27.5 |
| Skull 10 | 25.4 | 25.2 | 24.9 | 24.8 |
| Skull 11 | 25.9 | 25.4 | 25.3 | 25.6 |
| Skull 12 | 27.2 | 26.9 | 25.7 | 25.4 |
| Skull 13 | 25.3 | 25.8 | 26.2 | 26.5 |
| Skull 14 | 26.5 | 27 | 26.2 | 26.7 |
| Skull 15 | 24.7 | 25.2 | 25.1 | 25.5 |
CT: Computed tomography, FD: Fluid displacement
The comparison of the CT values of the right and left orbits for 15 skulls shows a mean of 0.3300 mm and a standard mean of 0.27757. The confidence interval ranges between −0.26532 and 0.92532. The t-value of the comparison is 1.189 and P = 0.254 was considered. The comparison of fluid displacement values of the right and left orbits was done and shows a mean of 0.4067 mm and a standard error mean of 0.2771. The confidence interval ranges between −0.1877 and 1.0011. The t and P-values of this comparison were 1.467 and 0.164, respectively. Hence, from the above values, we determined that there was no significant difference between the CT values of the right and left orbits and fluid displacement values of the right and left orbits.
The comparison of CT and real-time values of the right orbits shows a mean of 0.2333 mm and a standard error of 0.09794. The confidence interval ranges between −0.18673 and 0.23339. The t and P-values of this comparison were 0.238 and 0.815, respectively. The comparison of CT and real-time values of the left orbits shows a mean of 0/10011 mm and a standard error of 0.0981. The confidence interval ranges between −0.1104 and 0.3104. The t and P-values of this comparison were 1.020 and 0.325, respectively. Hence, from the above values, we determined that the CT values and the real-time values had no significant difference [Figure 4].

- Bar chart showing the minimum and maximum values of the computed tomography and fluid displacement values of the right and left orbits.
The scatter plots 1 and 2 [Figures 5 and 6] show that the linear pattern of distribution falls adjacent to the line of linearity of the observation of CT and real time on the right and left sides, respectively, which shows that the values of measurement are similar on skulls when comparing CT and real-time values.
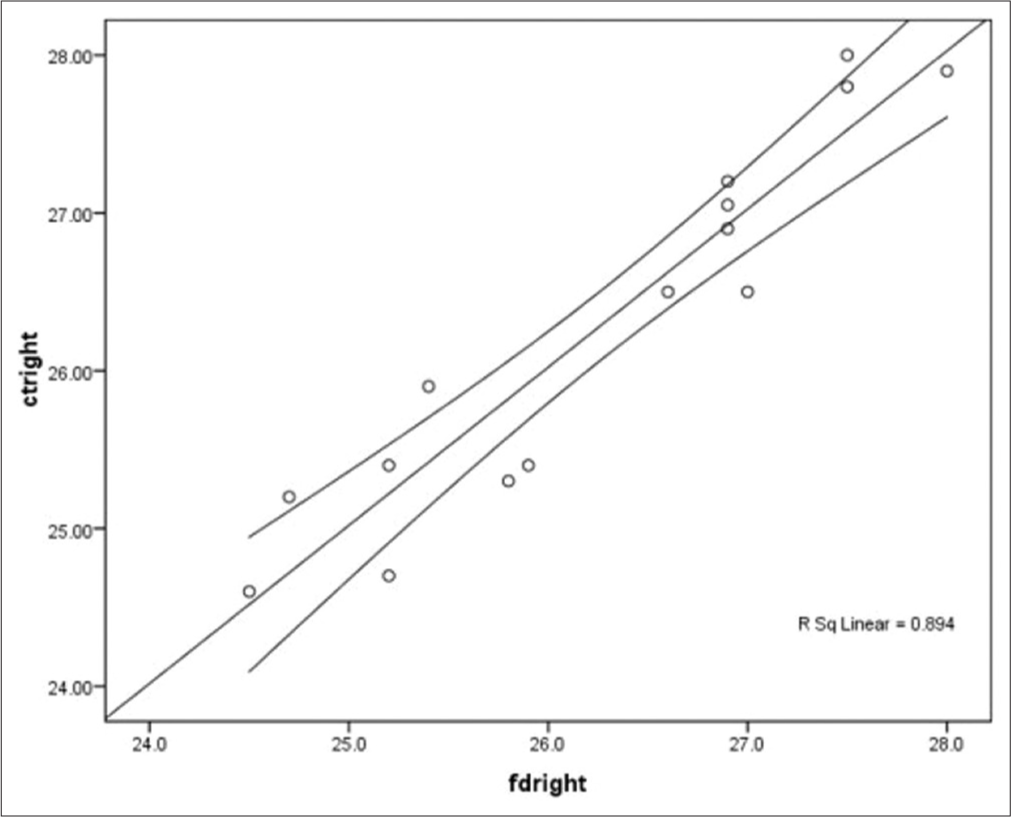
- Scatter plot comparison between the computed tomography and fluid displacement of the right orbit.
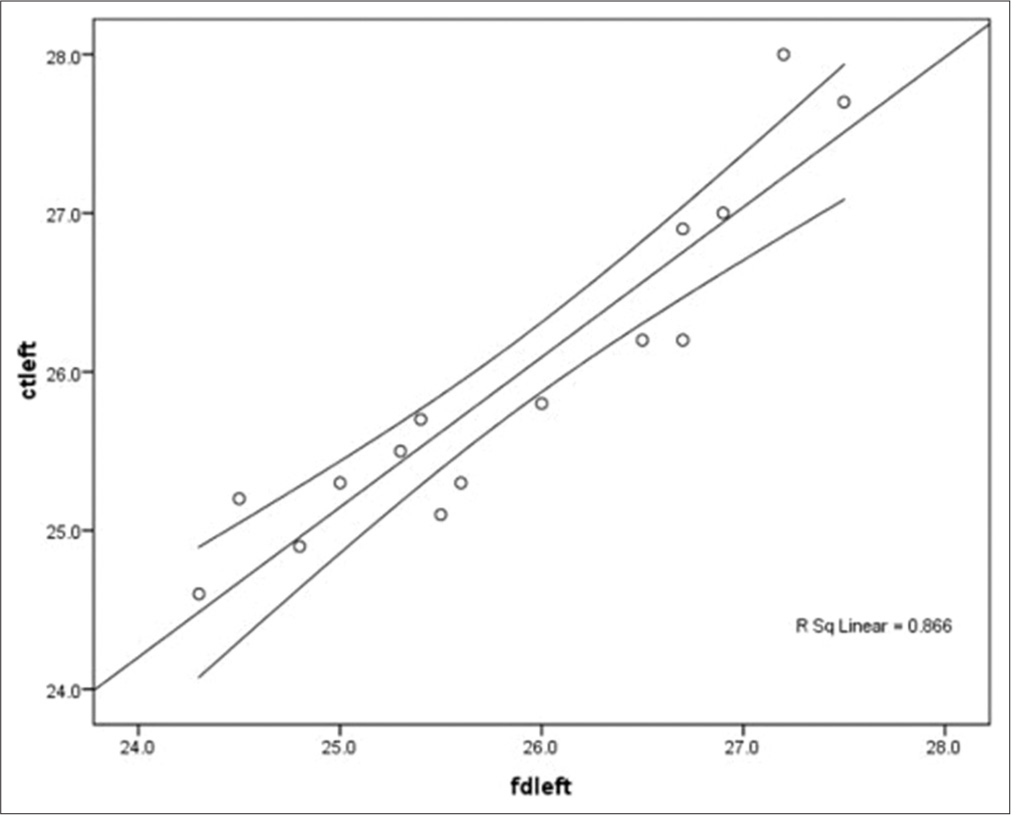
- Scatter plot comparison between the computed tomography and fluid displacement of the left orbit.
DISCUSSION
Facial bones are the eighth most common bones to be fractured in the human skeleton and on an average facial fracture reported to be 4.6/1000 cases. Orbital fractures account for 6.64% of all facial fractures.[9]
CT images have been extensively used as an investigation tool in orbital fractures and many studies by various authors were conducted to check the accuracy and refine the precision of CT scans. Following the studies conducted by Forbes et al., Sung et al., and Marsh and Gado, we concluded that the axial, sagittal, and coronal sections of the CT scans are mandatory for the orbital scanning to obtain a complete coverage of the orbital cavity.
Later, the measurement of the orbital volume using CT scans was introduced as most surgeons considered the orbital volume to be a very important factor in deciding the surgical intervention. Starting from a pixel counting technique to 3D reformation the software was refined for orbital volume measurement using CT.[10]
3D imaging has been very resourceful in reconstructive craniofacial surgery. Understanding of the abnormality is the first step toward reconstructive surgery of facial skeleton. Today in many medical centers, 3D images are considered essential before craniofacial surgeries. The morphological information provided by 3D CT images are valuable for the planning of exact surgical step (Vannier 17).
A wide range of software has been designed and applied for CT-based volumetric assessment over the years that have contributed significantly in this evolution and opened up scope for further research.[11-20]
Difference or not in the orbital volume between two sides has also been studied extensively on dry skulls.[21-25] Felding et al. in his study aimed at comparison of orbital volumes between the right and left sides found a difference of about 0.19 mm (24.42 mm on the right and 24.13 on the left). Ji et al.[26] conducted a similar study and found volume of the right side orbit to be 24.61 cubic mm and the left side to be 24.59 cubic mm. Forbes et al.[9] compared the right and left orbits where the right side orbital volume was 22.06 cubic mm and the left side orbital volume was 22.7 cubic mm. In our study, the mean orbital volume of the right side is 26.29± 1.16 cubic mm and that of the left orbit is 25.96± 1.025 cubic mm. The orbital volumes of both orbits were found to be significant and there is no statistical difference between the right and left sides on CT scans.
The difference in orbital volume between the two sides was 0.3 cubic mm which is similar to that observed in the previous studies and is negligible. One of the primary purposes of this study was to validate the authenticity of mirroring in reconstructive orbital surgery. This could be achieved by proving the existence of such negligible difference in orbital volumes between the right and left sides.
The CT scans had to be validated to find the accuracy of the CT and, hence, a real-time measurement of the orbital volume was done in a similar way as Forbes et al., Deveci et al., and Felding et al. using fluid displacement technique (Archimedes principle). The measurement of the orbital volume done using CT scans by Forbes et al. was 22.67 cubic mm (New York), Deveci et al. was 29.39 cubic mm (Turkey), Felding et al. was 24.27 cubic mm (Denmark), and our study showed a CT software mean orbital volume of 26.12± 1.09 cubic mm (Chennai).
The validation of the above CT values was then done by fluid displacement technique (Archimedes ’principle) using a mold of the orbit. Forbes et al.,[9] Deveci et al.,[19] and Felding et al.[25] used fluid displacement technique and estimated the orbital volume as 21.25 cubic mm, 28.37 cubic mm, and 24.27 cubic mm, respectively. In our study, the mean orbital volume using fluid displacement technique was found to be 26.06± 1.04 cubic mm.
In our study, the orbital volume difference between the software and the direct technique was 0.03 cubic mm in the right orbit and 0.1 cubic mm in the left orbit and, hence, proved that orbital volume measured by CT scan is very reliable and there is not much difference in the volume. It has also been confirmed that CT scan is a valuable, reliable, quick, and non-invasive tool to assess the orbital volume and it is a gold standard tool till date. It was also found that the left orbital volume is lesser than the right orbital volume by 0.33 cubic mm in CT scan and 0.4 cubic mm in fluid displacement thus stating that it is effective to compare the right and the left orbital volumes or mirror image it.
Limitations
Error in defining the anatomical boundaries during alginate impressions.
Error in marking the anatomy on software.
Person dependency (the same person has to define the anatomical boundaries and software to minimize error).
The CT scan and real-time volume should be taken on the same day within few hours of making the impression to avoid the impression shrinkage.
Accuracy in obtaining skull with intact bilateral orbits.
CONCLUSION
The results of the study confirm that orbital volume in native population remain predictable with values of 26.12± 1.09 cubic mm. Although the volume is not identical between sides, the difference of 3% is marginal and may be of lesser clinical significance. Our study also reiterates the fact that contralateral orbits can be used as digital benchmark for post-traumatic restoration of orbital volume.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Conflicts of interest
There are no conflicts of interest.
Financial support and sponsorship
Nil.
References
- Relative difference in orbital volume as an indication for surgical reconstruction in isolated orbital floor fractures. Craniomaxillofac Trauma Reconstr. 2011;4:203-12.
- [CrossRef] [PubMed] [Google Scholar]
- Orbital volume measurement in exophthalmos using a three dimensional CT imaging. Plast Reconstr Surg. 1985;75:502-8.
- [CrossRef] [PubMed] [Google Scholar]
- Pure orbital blowout fractures: New concepts and importance of medial orbital blowout fracture. Plast Reconstr Surg. 1999;103:1839-49.
- [CrossRef] [PubMed] [Google Scholar]
- Analysis and results of treatment of established post traumatic facial deformities. Plast Reconstr Surg. 1992;90:574-84.
- [CrossRef] [PubMed] [Google Scholar]
- An analysis of 2067 cases of zygomatico-orbital fractures. J Oral Maxillofac Surg. 1985;43:417-28.
- [CrossRef] [Google Scholar]
- Compuer-assissted orbital volume measurement in the surgical correction of late exophthalmoss caused by blowout fractures. Ophthal Last Reconstr Surg. 2003;19:207-11.
- [CrossRef] [PubMed] [Google Scholar]
- Effectiveness of secondary post-traumatic periorbital reconstruction. J Craniomaxillofac Surg. 1995;23:143-50.
- [CrossRef] [Google Scholar]
- Dimensions and volume of the orbit and orbital fat in post-traumatic enophthalmos. Dentomaxillofac Surg. 2000;29:302-11.
- [CrossRef] [Google Scholar]
- Volume measurement of normal orbital structures by computed tomographic analysis. AJR Am J Roentgenol. 1985;145:149-54.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of exophthalmos by computer based volume measurement of orbital fractures in a Korean population. Ophthalmic Plast Reconstr Surg. 2007;24:36-9.
- [CrossRef] [PubMed] [Google Scholar]
- Measurements of orbital volume change using computed tomography in isolated orbital blowout fractures. Arch Facial Plast Surg. 2009;11:395-8.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative computed tomography for evaluation of orbital volume change in blow-out fractures. J Formos Med Assoc. 1993;92:349-55.
- [Google Scholar]
- Incidence of fractures in a geographically defined population. J Epidemiol Community Health. 1990;44:241-5.
- [CrossRef] [PubMed] [Google Scholar]
- Orbital volume measured by a low-dose CT scanning technique. Dentomaxillofac Radiol. 1992;21:70-2.
- [CrossRef] [PubMed] [Google Scholar]
- Studies on enophthalmos: II. The measurement of orbital injuries and their treatment by quantitative computed tomography. Plast Reconstr Surg. 1986;77:203-14.
- [CrossRef] [PubMed] [Google Scholar]
- The longitudinal orbital CT projection: A versatile image for orbital assessment. Plast Reconstr Surg. 1983;71:308-17.
- [CrossRef] [PubMed] [Google Scholar]
- Model based segmentation in orbit volume measurement with cone beam computed tomography an evaluation against current concepts. Int J Comput Assist Radiol Surg. 2016;11:1-9.
- [CrossRef] [PubMed] [Google Scholar]
- Three dimensional CT reconstruction images for craniofacial surgical planning and evaluation. Radiology. 1984;150:179-84.
- [CrossRef] [PubMed] [Google Scholar]
- Measurement of orbital volume by a 3-dimensional software program: An experimental study. J Oral Maxillofac Surg. 2000;58:645-8.
- [CrossRef] [Google Scholar]
- Measurement of orbital volume after enucleation and orbital implantation. PLoS One. 2012;7:e50333.
- [CrossRef] [PubMed] [Google Scholar]
- A computer-based method for calculation of orbital floor fractures from coronal computed tomography scans. J Oral Maxillofac Surg. 2001;59:1437-42.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation of computer-based area and volume measurement from coronal computed tomography scans in isolated blowout fractures of the orbital floor. J Oral Maxillofac Surg. 2002;60:1267-72.
- [CrossRef] [PubMed] [Google Scholar]
- Prediction of enophtamos by computed tomography after blow out orbital fractures. Br J Ophthalmol. 1994;78:618-20.
- [CrossRef] [PubMed] [Google Scholar]
- Retrospective study maxillofacial fractures epidemiology and treatment plans in Southeast of Iran. Med Oral Patol Oral Cir Bucal. 2015;20:e729-36.
- [CrossRef] [PubMed] [Google Scholar]
- The Dimensions of the orbital cavity based on high-resolution computed tomography of human cadavers. J Craniofac Surg. 2016;27:1090-3.
- [CrossRef] [PubMed] [Google Scholar]
- Quantitative morphometry of the orbit in Chinese adults based on a three-dimensional reconstruction method. J Anat. 2010;217:501-6.
- [CrossRef] [PubMed] [Google Scholar]




