
Translate this page into:
Double obstruction of upper and lower urinary tract in a child due to renal stone disease: Endoscopic treatment
*Corresponding author: Sangeetha Geminiganesan, Department of Paediatric Medicine, Division of Paediatric Nephrology, Sri Ramachandra Institute of Higher Education and Research, Chennai, Tamil Nadu, India. sangeethaperungo@gmail.com
-
Received: ,
Accepted: ,
How to cite this article: Geminiganesan S, Ravichandran L, Srinivasan RB. Double obstruction of upper and lower urinary tract in a child due to renal stone disease: Endoscopic treatment. Sri Ramachandra J Health Sci 2021;1:31-3.
Abstract
Incidence of renal stone disease/urolithiasis has increased significantly in children due to multifactorial causes. Stones secondary to metabolic abnormalities are treatable if it is identified at the early stage. Surgical intervention may be needed depending on the site, size of the stone, and the clinical presentation. We report a 12-year-old adolescent boy with multiple calculi at various sites who needed medical as well as surgical intervention.
Keywords
Renal stone disease
Hypercalciuria
lithotripsy
Urinary tract obstruction and ureterorenoscopy

INTRODUCTION
Incidence of pediatric renal stone disease (RSD)/urolithiasis is on the increasing trend. Potential exogenous causes are reduced water intake, excess salt and fructose consumption, obesity, and rise in ambient temperature. Endogenous factors include familial/idiopathic hypercalciuria, hyperoxaluria, hypocitraturia, hyperuricosuria, cystinuria, renal structural malformations (medullary sponge kidney, autosomal dominant polycystic kidney disease, pelvi-ureteric junction obstruction, horseshoe kidney, and calyceal diverticula), ketogenic diet, drug-induced stones, and urinary infection with urease producing organisms.[1,2] Here, we report a 12-year-old boy with primary hypercalciuria and double obstruction due to multiple calculi.
CASE REPORT
A 12-year-old developmentally normal male child presented with acute severe abdominal pain and vomiting of 2 days duration. He had typical strangury, a symptom characterized by painful incomplete voiding. There was no history of fever, hematuria, or passage of stone in urine. Family history was negative for RSD. On examination, his vitals, nutritional status, and growth parameters were appropriate for age. He had severe tenderness over the left loin and supra pubic region. Working diagnosis of renal colic was made. X-ray abdomen showed nephrocalcinosis, multiple bilateral tiny renal calculi, left proximal calculus, and a calculus at prostatic urethra [Figure 1]. Ultrasound abdomen revealed renal calculi of varying sizes on both kidneys with evidence of nephrocalcinosis [Figure 2]. There was left hydroureteronephrosis due to the left proximal ureteric stone and bladder distension due to prostatic urethral stone.
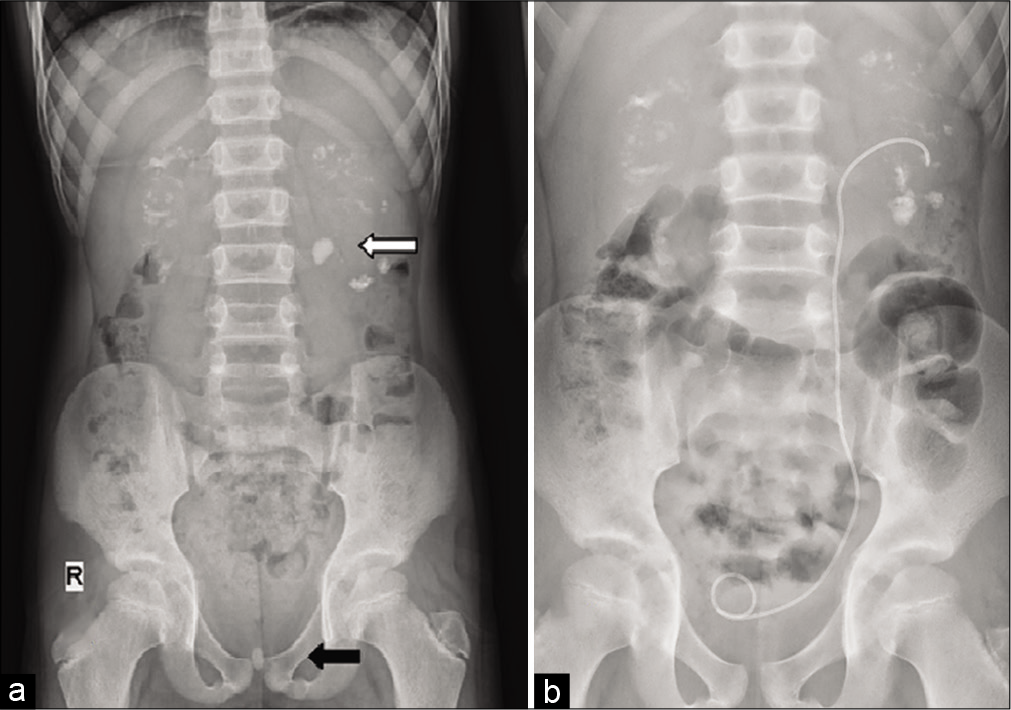
- (a) X-ray abdomen showing bilateral multiple renal calculi with nephrocalcinosis. White arrow points to the proximal calculus causing obstruction to the left upper tract. Black arrow points to the prostatic calculus causing bladder outlet obstruction in the same patient. (b) post op image showing stent in situ after clearance of obstructing calculi at PUJ and bladder outlet.
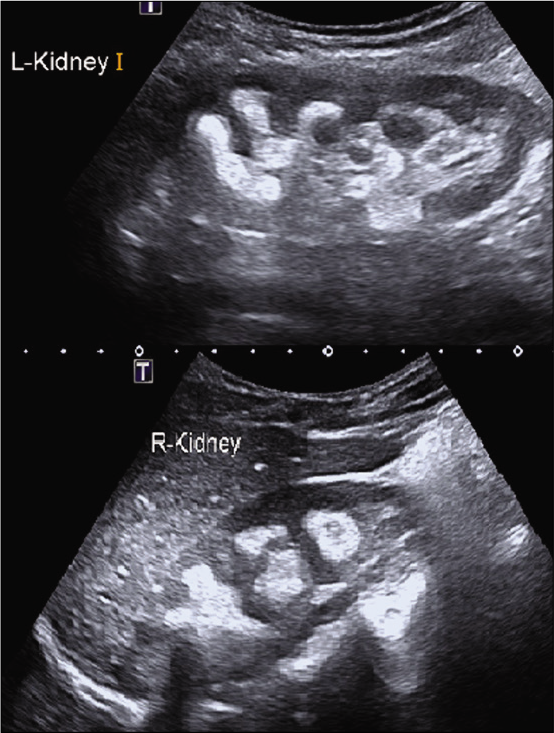
- USG abdomen showing multiple bilateral renal calculi with evidence of nephrocalcinosis.
All metabolic work up including renal function test, serum calcium, intact parathyroid hormone, uric acid, magnesium, and urine routine were normal. Urine culture was sterile. Twenty-four hours urine for oxalate and uric acid were within limits. Significant hypercalciuria of 13 mg/kg/day was noted.
Since he was symptomatic with obstructive feature, he was taken up for endoscopic treatment. The prostatic urethral calculus was pushed into the bladder with pediatric cystoscope and fragmented using laser lithoclast. Using 4.5/6 F pediatric uretero renoscope, the left upper ureteric calculus was broken using laser energy [Figure 3]. Good stone clearance was achieved and a DJ stent was kept for 6 weeks. Crystallographic analysis of the stone fragments showed calcium oxalate monohydrate (57%) and dihydrate (32%). He was started on hydrochlorothiazide 0.5 mg/kg/day. He has been advised to take reduced salt diet and water intake of 3 liters/day to ensure urine output of more than 2 liters/day.
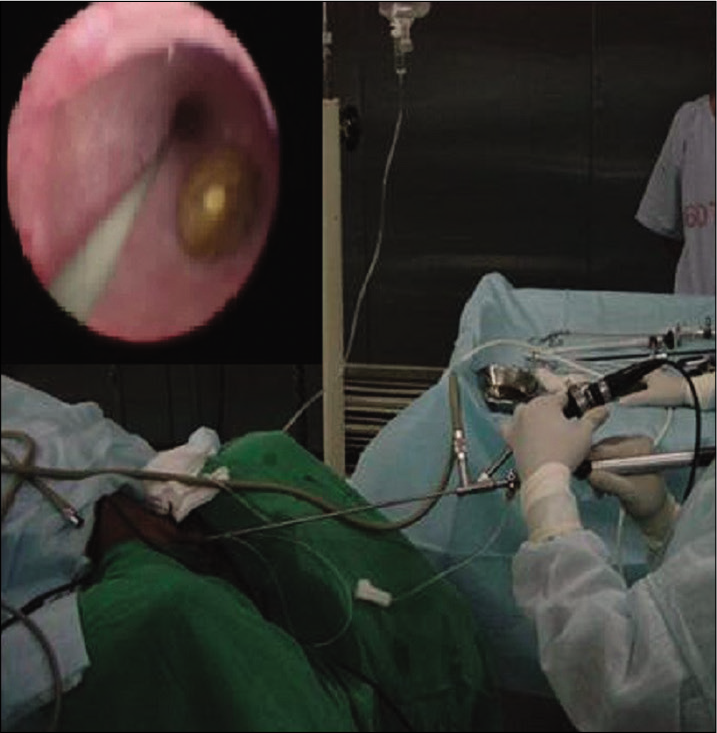
- Ureterorenoscopy and lithoclast of ureteric stone.
DISCUSSION
The diagnosis of RSD in children has doubled from 7.2 to 14.5/100,000 person-years in the past 2 to 3 decades.[3,4] Colicky abdominal pain is the most common presentation of stone disease (50–80%) followed by non-specific abdominal pain and gross hematuria in 30–50% children. Lower urinary tract symptoms such as frequency, urgency and dysuria, urinary tract infection, urinary retention in case of stone obstructing the urethra, and passage of stones are the other common presentations. At the extreme, repeated stone formation can also present with acute kidney injury and chronic kidney disease and end stage renal failure. Ameen et al. showed that urethral calculi are more common in adult male and prostatic urethra is the most common site. In his study, out of 63 patients, only 19% were children and all were males.[5]
Risk factors for stone disease are generally being identified in 75–85% of children. They include urinary metabolic abnormality (40–50%), structural urinary tract abnormality, and urinary tract infection.[6,7] Excess solutes such as calcium, oxalate, uric acid, and cystine in urine with low urine volume led to solute supersaturation and crystals formation. Decreased levels of citrate, magnesium, and pyrophosphate which are natural inhibitors of stone formation are an added factor. The most common metabolic abnormality identified in pediatric age group is hypercalciuria and it is defined as urinary calcium excretion >4 mg/kg/day in a child greater than 2 years of age, on a routine diet.[8,9] Increased intestinal absorption, renal excretion, or bone resorption are the possible contributing mechanisms. This child had hypercalciuria with normal serum calcium; hence, renal hypercalciuria was considered as the probable etiology. Acute renal colic is usually managed with good hydration therapy, paracetamol with or without NSAIDs after ensuring normal renal function.
Spontaneous passage of calculus is possible if the size is <5 mm. Indication for surgical intervention includes symptomatic stone which is not responding to conservative therapy, stone with obstructive features, and size >6 mm. Since this patient had a ureteric and urethral stone size of 8 mm with hydroureteronephrosis, he underwent endoscopic lithotripsy. For upper and mid ureteric stones, ureterorenoscopy with laser/pneumatic lithotripsy is preferred. Percutaneous nephrolithotomy is needed for larger stones in pelvi calyceal system. Adequate fluid intake is a key component to prevent stone recurrence. Low sodium diet and hydrochlorothiazide should be started in children with hypercalciuria to prevent recurrent stones.[10]
CONCLUSION
The presence of upper and lower ureteric obstruction (double obstruction) in same patient is rare. Latest pediatric uretero renoscopy and laser lithoclast enable management of multiple calculi in same sitting as in our case. Metabolic work up and prompt medical treatment are essential to prevent stone recurrence in children.
Acknowledgment
We acknowledge the staff nurses of paediatric medicine department for the care of this child.
Declaration of patient consent
The authors certify that they have obtained all appropriate patient consent.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- Pediatric urolithiasis: Causative factors, diagnosis and medical management. Nat Rev Urol. 2012;9:138-46.
- [CrossRef] [PubMed] [Google Scholar]
- Urolithiasis in children In: Avner ED, Harmon WE, Niaudet P, Yoshikawa N, Emma F, Goldstein SL, eds. Pediatric Nephrology (7th ed). Berlin, Heidelberg: Springer; 2016. p. :839-82.
- [Google Scholar]
- Temporal trends in incidence of kidney stones among children: A 25-year population based study. J Urol. 2012;188:247-52.
- [CrossRef] [PubMed] [Google Scholar]
- Comparison of risk factors for pediatric kidney stone formation: The effects of sex. Front Pediatr. 2019;7:32.
- [CrossRef] [PubMed] [Google Scholar]
- Evaluation and management of urethral calculi. Int Surg J. 2017;4:2392-6.
- [CrossRef] [Google Scholar]
- Epidemiology of paediatric renal stone disease in the UK. Arch Dis Child. 2003;88:962-5.
- [CrossRef] [PubMed] [Google Scholar]
- Nephrolithiasis and nephrocalcinosis in childhood-risk factor-related current and future treatment options. Front Pediatr. 2018;6:98.
- [CrossRef] [PubMed] [Google Scholar]
- Urinary metabolic evaluations in solitary and recurrent stone forming children. J Urol. 2008;179:2369-72.
- [CrossRef] [PubMed] [Google Scholar]
- Urine risk factors in children with calcium kidney stones and their siblings. Kidney Int. 2012;81:1140-8.
- [CrossRef] [PubMed] [Google Scholar]
- Low-dose thiazide diuretics in children with idiopathic renal hypercalciuria. Acta Paediatr. 2011;100:e71-4.
- [CrossRef] [PubMed] [Google Scholar]




